乳腺密度尺显示不同程度的乳腺密度。Image courtesy of Robert L. Bard, M.D.
Prologue
In 2014, Imaging Technology News (ITN) introduced breast cancer survivor-turned-crusaderNancy Cappello, Ph.D., and her story about having dense breast tissue leading to a late-stage cancer. A false negative mammography scan (diagnosed in 2004) concealed a large 2.5 cm suspicious lesion, which was later confirmed to be stage 3c breast cancer. This same cancer had metastasized to 13 lymph nodes. This sparked Cappello to create the“Are You Dense?” Foundation-一场提高国际意识的运动,以更好地支持乳腺密度诊断,并倡议通过立法来颁布法律,要求乳房x光检查中心告知患者乳房密度和相关的癌症风险。Cappello2018年11月15日,她因继发性骨髓增生异常综合征(MDS)去世,这是一种骨髓癌,是她之前积极的乳腺癌治疗的并发症。但她点燃了为改善政策、成像技术和先进研究而斗争的遗产,以更好地解决这一健康危机,估计有40%的女性人口(乳房致密的女性)处于错误的阴性读数的风险。
***
In a recent clinical study co-investigated byRobert Bard, M.D., andNoelle Cutter, Ph.D., data is collected from a cohort of women undergoing ultrasound density scans. Inspired by Nancy Cappello’s early surveys of specific demographic groups, this 2021 research exploresdense breastpredominance in the younger population or those with lower body mass index (including dancers and athletes). Both are likely candidates to receive false negative readings on a mammogram.
此外,在40-65岁的女性中,乳房密度也与患乳腺癌的风险有关,但有有限的证据表明,它与18岁以上女性患乳腺癌的风险有关。This estimated proportion of breast cancers are attributable to breast cancer risk factors commonly documented in clinical practice and used in breast cancer risk prediction models, includingBI-RADSbreast density and ultrasounds to confirm mammography readings.
Target Objectives
Endurance athletes are to be defined by those who participated in one or more endurance events (long course) in the year or as well as those who are younger, with a low BMI, and had the classification of “dense breasts.” This was heterogeneous and extremely dense as noted by the BI-RADS code (heterogeneouslyor extremely dense vs.scattered fibroglandular densities). Data is collected as odds ratio (ORs) and 95 percent confidence intervals included in research outcomes.
虽然乳房密度是一个公认的和普遍的乳腺癌风险因素,但它的生物学联系尚不清楚。需要更多的研究来支持绝经前运动妇女与人群相关的风险比例。从这项研究中收集的数据回顾了一组接受超声成像扫描的绝经前致密乳房的女性。有趣的是,50年前,人们从未见过一个35岁的人患乳腺癌。20年前,20多岁的女性患癌症很常见。环境因素和有毒物质的致癌效应可能是研究结果的副产品。
Non-invasive Imaging Options
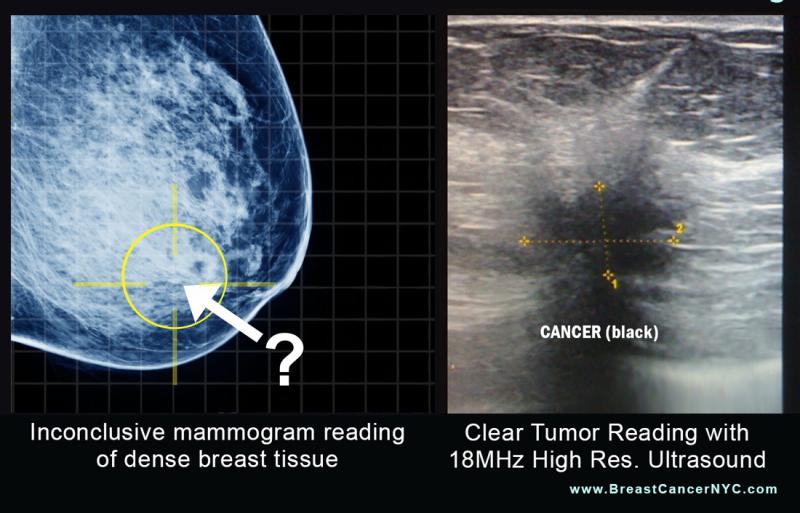
1.Diagnostic Ultrasound.诊断超声满足扫描要求,并且由于当今超声设备的高分辨率和低成本,可以在办公室环境中准确、快速地进行。此外,计算机化成像、血流和肿瘤精确体积和血管密度的测量的进步现在不那么依赖于操作者,增加了这项或任何需要使用超声技术的临床研究的易用性。这提供了一种可靠的和可重复的诊断,以及一种跟踪个人癌症发展、进展和治疗反应的独特模式的手段。
Recent technological advances also make these procedures available to much broader clinical application, without requiring years of very unique training and clinical experience, for example, with diagnoses of cystic versus solid lesions. Accuracy in assessing breast1 tumors and metastatic foci has been documented. It must be emphasized that the beginner will find many confusing artifacts and findings should be confirmed with all pertinent imaging modalities.
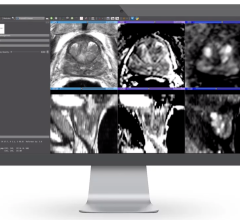
2. 3-D Doppler Ultrasound With Dynamic Contrast Enhanced MRI.These are the gold standards by which cancers are initially diagnosed or confirmed and serially followed after treatment. The percentage of malignant vessels can be quantified and re-evaluated in the identical tumor volume as serial follow ups to the standard treatments using radiation, surgery, hormones, chemotherapy, cryotherapy, watchful waiting and the non-standard regenerative treatments: ablation using focal laser, focal ultrasound, photodynamic, radiofrequency and microwave technologies. Since vessel mapping is possible, embolic treatments may be considered.
3. 3-D Sonography.3-D sonography can demonstrate the tumor volume and marginal capsule of locally affected lymph nodes more accurately than the MRI since the resolution is 100 microns at 18 MHz. The exam takes about 10 minutes, and the probes are automated, meaning that this is less operator dependent than other sonographic procedures. Vessel density index (VI) imaging is performed on the dataset at an independent workstation and comparison made with prior exams if available.
4. 3-D Power Doppler.三维能量多普勒指数根据肿瘤的分期、组织学分级、包膜破坏和淋巴结转移的不同而不同。组织学分级已经用该技术进行了研究,以下近似方法在前列腺肿瘤分期中被证明是有用的。这种新生血管的定量测量最初应用于前列腺癌虽然它与组织学格里森分级并不完全相关,因为这是一种当前的功能测量,而显微镜纯粹是解剖学的,可能不能代表当前的攻击潜力,但它的攻击预测价值可以在乳腺癌和其他癌症的背景下进行研究。3, 4
Medical imaging can map the arteries, veins and nerves providing pre-operative landmarks reducing post-operative bleeding and avoiding nerve damage. Tumors of low aggressive potential may be treated medically and followed by interval scans or locally reduced by radiation or laser ablation. Biopsies of certain abnormalities may be averted or postponed.(See Figure 1.)
Tracking Breast Cancers and Tumors
High tumor vessel density correlates with greater aggression. Axillary and mediastinal imaging can document lymphadenopathy. Abdominal scans simultaneously performed may detect ascites and metastases to the liver, periaortic nodes and pelvic organs. Response to neoadjuvant chemotherapy may be assessed with MRI, CT, mammography, PET/CT and ultrasound. The new technology of ultrasound elastography, assessing tumor stiffness, predicts response to treatment accurately and may indicate better therapeutic strategies on a timelier basis.5 Residual cancer burden scoring could provide better treatment options since the treatment response for evaluation of neoadjuvant chemotherapy needs a more comprehensive and authoritative standard than is currently available.
Lymph Node Disease
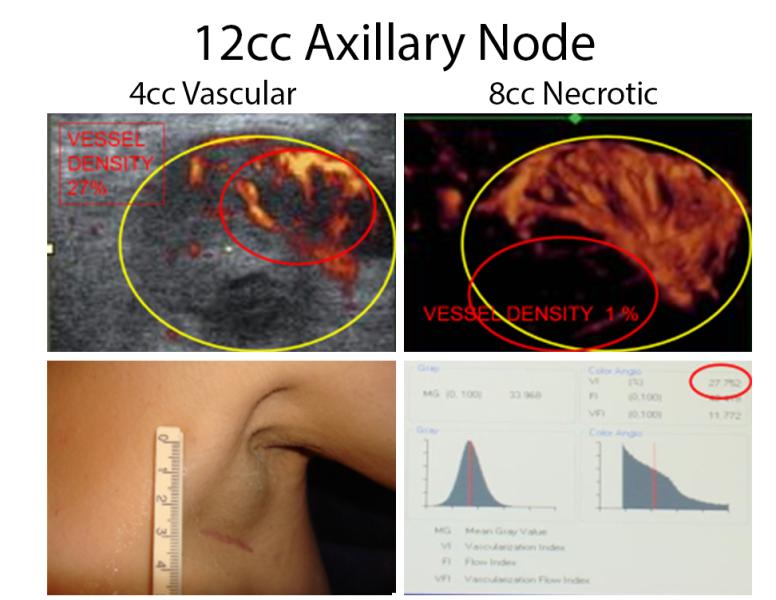
淋巴结评估是可能的同时。在超声引导下,可进行活检。恶性肿瘤的超声标准已在其他地方发表。肿大淋巴结的图像引导可以区分活动性肿瘤和坏死区域,减少对不确定结果重复期望的必要性。(See Figure 2.)Pathologic assessment of a large post-operative specimen may be facilitated by high frequency scanning to re-localize the suspect region for targeted study that has been removed from its previous anatomic position.6Elastography is useful in targeting sub-centimeter foci in large nodal masses.
Image-guided Biopsy and Treatment
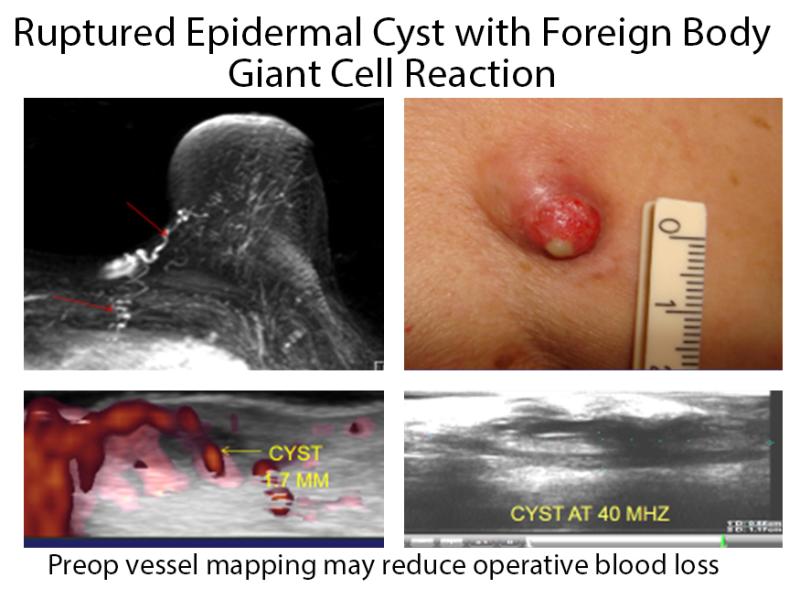
新的计算机程序使用纳米技术和控制模式进行精确的图像引导活检和治疗选择。在14mhz以上的频率下,小至3mm的病灶已成功成像。利用三维超声多普勒,医生手动定位最高肿瘤新生血管区域。这是至关重要的,因为只有部分肿块可能是癌变的,在非靶向穿刺活检中可能会漏诊。MRI与超声的结合使得图像引导下的活组织检查可以避免相邻的血管通道。同样的技术允许在局部麻醉下进行定制的超声或mri引导的活组织检查。立即对肿瘤细胞进行细胞学检查,可以取出活检针,插入激光纤维或低温探针,立即治疗已证实的肿瘤。核磁共振热偶传感器可以防止邻近神经和敏感组织过热。消融后,通过多普勒、对比超声或DCE-MRI确认破坏区域。深入的炎症病灶可通过机器人图像引导下皮下注射或必要时进行靶向活检。 This outpatient procedure allows the patient to return to work immediately. RF thermoprobes with temperature auto cutoffs prevent thermal skin damage.7 Similar user-friendly and cost-effective modalities may replace other therapies in the near future. At the 2016 American Society of Lasers in Medicine (ASLMS) meeting in Boston, cutaneous melanoma with in-transit metastases was successively treated by laser technologies,8 MRI fusion biopsies with CT and/or ultrasound are routine adding further to the accuracy of image-guided biopsies and focal treatment procedures.9(See Figure 3.)
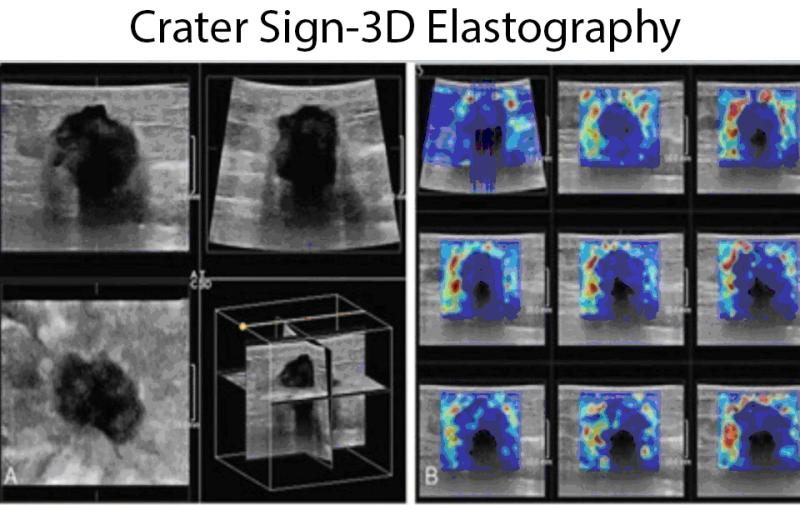
Advances in ultrasound elastography progressed from simple strain imaging to shear wave sonography, to 3-D coronal shear wave elastography where the plane of the image corresponds to the surgical field as the tumor is dissected in the most superficial plane. The tumor desmoplasia in the coronal plane creates a sawtooth irregular border with a central echo pattern simulating a “donut” and is termed the “crater” sign in this increasingly popular imaging paradigm. Elastography is used worldwide primarily in the diagnostic workup of breast, thyroid and prostate tumors, and has reduced the number of biopsies on false positive findings from mammography, b-mode ultrasound and MRI.10
Robert L. Bard, M.D., PC, DABR, FASLMS,是癌症诊断成像中心(NYC)的活跃医学主任,使用先进的三维超声多普勒成像来检测乳腺癌,前列腺,皮肤,甲状腺,黑色素瘤和其他区域的癌症。He has extensive credentials as a clinical researcher/validator and has published medical textbooks and science journals.
Noelle L. Cutter, Ph.D.她是莫洛伊学院的临时副院长,生物和化学教授,研究髓母细胞瘤(小儿脑癌)的免疫学和治疗方案的癌症研究员。
he is also an “Iron-Man” race winner and dedicated triathlete.
References:
1. Bard R. Vascular imaging of cancer in the dense breast. 60th Journees Francaises de Radiologie 2012, Paris
2.https://www.breastcancer.org/symptoms/understand_bc/statistics
3. Cruwys, Cheryl, and JoAnn Pushkin. “Breast density and impacts on health.” ecancermedicalscience 11 (2017).
4. Nazari, Shayan Shaghayeq, and Pinku Mukherjee. “An overview of mammographic density and its association with breast cancer.” Breast cancer 25.3 (2018): 259-267.
5. Boyd, Norman F., et al. “Mammographic density: a heritable risk factor for breast cancer.” Cancer epidemiology. Humana Press, 2009. 343-360.
6. Burton, Anya, et al. “Mammographic density and ageing: A collaborative pooled analysis of cross-sectional data from 22 countries worldwide.” PLoS medicine 14.6 (2017): e1002335.
7. Azam, Shadi, et al. “Determinants of mammographic density change.” JNCI Cancer Spectrum 3.1 (2019): pkz004.
8. Boyd, Norman F., et al. “Body size, mammographic density, and breast cancer risk.” Cancer Epidemiology and Prevention Biomarkers 15.11 (2006): 2086-2092.
9. Bard R. Image guided cancer treatment. Advances in Medical and Surgical Dermatology, 15th Annual Mt Sinai Winter Symposium New York 2015.
10. Merce L, Alcazar J, Lopez C et al. Clinical usefulness of 3-dimensional sonography and power Doppler angiography for diagnosis of endometrial carcinoma. J Ultrasound Med 2007; 26:1279-1289.
Click through the links below to see ITNtv interviews with Cappello, as well as pieces she contributed to the magazine.
VIDEO: The Impact of Breast Density Technology and Legislation
VIDEO: Personalized Breast Screening and Breast Density
VIDEO: Breast Cancer Awareness - Highlights of the NCoBC 2016 Conference
Fake News: Having Dense Breast Tissue is No Big Deal
The Manic World of Social Media and Breast Cancer: Gratitude and Grief



 August 11, 2022
August 11, 2022