In a detailed overview held during theRadiological Society of North America’s (RSNA) 2021 annual meeting, promising results from an Institutional Review Board (IRB)-approved study were presented byGeorgia Giakoumis Spear, MD.She serves as chief of the department of2022世界杯篮球预选赛赛程withNorthShore University HealthSystem, and is an associate professor of radiology at theUniversity of Chicago Pritzker School of Medicine.
NorthShore University HealthSystem includes four hospital-based full-service comprehensive breast centers and five satellite imaging centers. A teaching affiliate at the University of Chicago, it has 14 board certified radiologists specializing in breast imaging. The high-risk breast clinic, part of theKellogg Comprehensive Cancer Center该公司每年提供95,000张筛查性乳房x光片,医生负责所有诊断性超声波检查。
In the session, Spear, who uses theGE Invenia ABUS 2.0 system, shared the benefits of addingwhole breast automated ultrasound(ABUS) screening to clinical practice, enhancing cancer detection in dense breast tissue. Featuring case-based review, the presentation included strategies for successful implementation and interpretation.
QView Medical而且GE Healthcare announced, in November 2021, that QView’sQVCADsoftware can be launched on GE Healthcare’s Invenia ABUS 2.0, the first FDA-approved ultrasound supplemental breast screening technology specifically designed for detecting cancer in dense breast tissue.
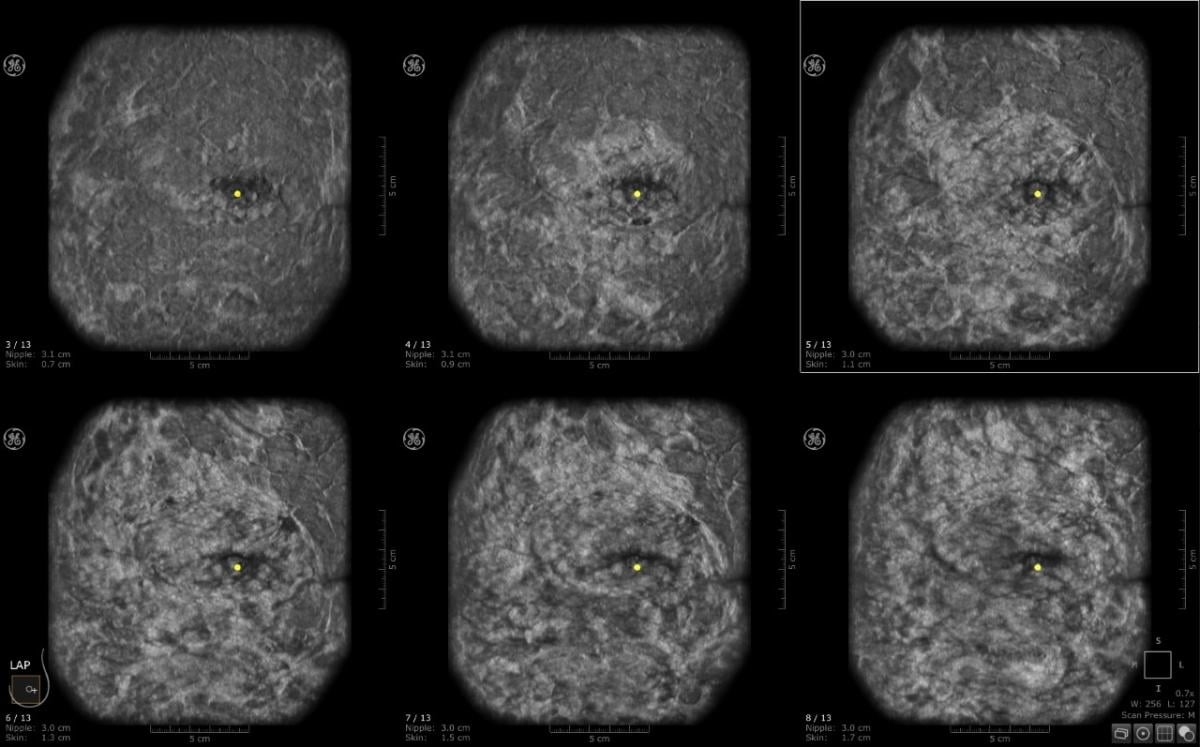
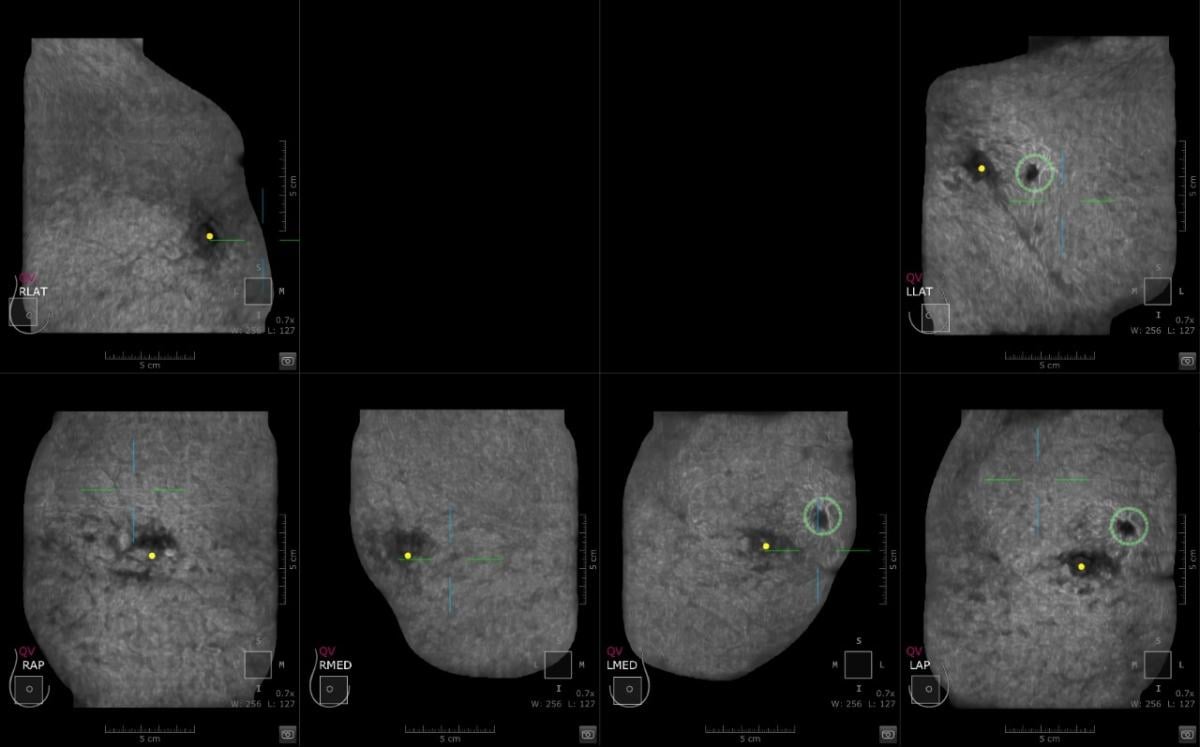
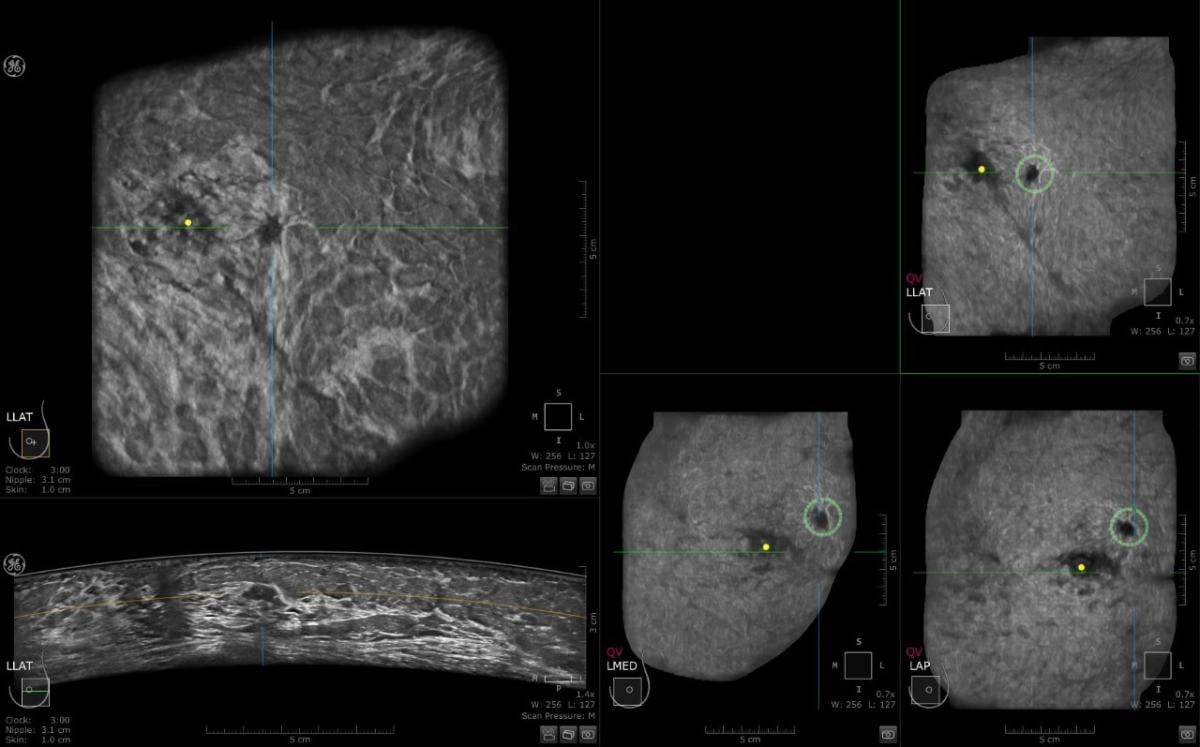
This is a case where CAD detected an abnormality in the left breast and the margins are irregular. Multiview display. QView CAD detection integrated in the ABUS. Bilateral breast ABUS display with the pink indicator indicating that QView CAD is processed. Image courtesy of Georgia Giakoumis Spear, MD
ABUS: Why and How We Use It
In providing an overview of ABUS, its uses and benefits, and the clinical study, Spear offered reasons why ABUS is a valuable solution for central screening with breast tissue. She noted that breast density limits the ability to detect breast cancer, which can impact a woman’s risk 4-6 fold. She applauded progress with mandatory breast density legislation, noting that, as of 2021, a total of 38 states and DC are following legislation, and 8 have supplemental screening reimbursement legislation, reflective of an Increased demand for supplemental screening.
“The onus is on us to find those cancers,” stated Spear. Speaking to the effectiveness of the new technology available, she added, “You can’t help but make believers of these advances (in reference to QView’s CAD technology), because we are finding things that we’d not seen before.”
In an overview of the NorthShore University HealthSystem Retrospective IRB-approved Study, she noted that this was a study of the first 500 patients who underwent ABUS for supplemental screening. Results included 6 small, invasive, node-negative, clinically significant breast cancers detected (CDR 12/1,000); a low call back rate of <10%, and a 55% high positive biopsy rate. She noted that this was a 3-year prospective clinical trial, recently completed, compiling of data ongoing. The high CDR and low recall rates were attributed to four factors:
• Facility with ultrasound in the practice;
• incidence vs. prevalence screens;
• image quality optimization; and
• interpretation strategies.
转诊来自他们自己的放射科医生和技术人员;高危乳腺门诊;乳房手术部门;并咨询医师。
Eligibility criteria was as follows:
•Patients withBI-RADSdensity
categories C&D;
•difficult clinical examination; and
•current mammogram (within 9 months).
At NorthShore University HealthSystem, Spear and her colleagues work with theQView CADapplication, which can be accessed through the Invenia ABUS 2.0 Viewer software from GE Healthcare. Spear shared detailed and promising outcomes she has experienced in the implementation process, noting that computer assistance detected abnormalities that may not have been caught initially. AI allows for analysis of hundreds of images and presents them in a single page via the QView CAS Navigator Image (3D map).
When AI was integrated into the reading workflow, in a review of 2,000 images with the QView CAD system, the results included a 33% reading time improvement, and a 93% sensitivity with 0.1 FPR per volume.
“You cannot help but make believers of people by showing these results,” she noted, adding, “This will help us improve both efficiency and success, offering wonderful specificity and sensitivity for new and experienced users.” She said this will help the radiologist look at three mammograms and add supplemental modality with thousands of images. Her experiences have led her to be a firm believer in the value of ABUS systems as an important element in busy practices, and is aware that having “distortions and lesions pop” is a benefit to radiologists and patients.
Clinical Implementation of ABUS
Spear addressed the practical benefits to radiology teams and summarized how the implementation process evolved for their team.
“There are many advantages on the horizon, especially given our increasingly busy practices, which often have us viewing 150-200 exams/day,” said Spear.
“Optimal input necessary for optimal output,” she added, reinforcing that “Image quality optimization was the key factor in successful interpretation.” Spear addressed the success factors for ABUS implementation include a team approach, communication, focusing on education, training, knowledge of displays, and strategies for interpretation. Here, then, an abridged summary of her presentation:
“We looked into automated ultrasound technology as we noticed the prevalence of dense breast tissue. In November 2015, we started performing this with two ABUS units, and now have 9 total, as we have found it to be both a physician satisfier and a patient satisfier. As an ultrasound facility, we wanted to learn why detection was high and call back rate was low.
“When we implemented automated ultrasound, we identified the patients who would most benefit … the goal was to reduce false positives and look for the cancer that they may have missed with justmammography.
“It was determined that the mammogram and automated breast ultrasound should both be done on the same day,” said Spear, who offered multiple benefits in doing so:
•Target areas of subtle mammographic question, focusing on same area in >2,000 ultrasound images.
•Combined assessment may minimize false positives on both studies and may increase combined accuracy of both exams.
•Eliminate need for callback from mammogram (i.e. new mammographic mass may be explained by cyst on same day ABUS).
Spear shared the top issues radiology teams need to consider with a new modality to establish success:
•Understanding physician staffing
• Technologist proficiency
• IT integration is crucial (large storage capacity is essential)
•Scheduling appropriate times and throughput in dept
•Coordination of interpretation
•Training with standardized protocols in small groups
斯皮尔说:“我们的目的是找到更多的癌症,这将帮助他们更成功。”“手持式和自动化有很大的不同,自动化可以看到冠状面,这是成功的关键。”
Spear listed some advantages of automated ultrasound over handheld ultrasound:
•Reproducibility and consistency
•Easy to perform, does not require physician time to perform
•Consistent image acquisition time
•Reduces expected delays, allows streamlined workflow
•Physician time for interpretations decreases with experience
•Post processing advantages
•Coronal views helpful in detecting architectural distortion
•Sharper images
•Large area of coverage
ABUS Scanning and the Benefits of the Unique Coronal Plane
Spear discussed that this acts as a roadmap for evaluation of the breast and allows for anatomic consistency. It also shows a breast’s radial anatomic arrangement, and the wide footprint allows for longer area of breast tissue coverage with one scanning motion. Extended field of view allows for evaluation of multiple findings and larger area of tissue surrounding a lesion, and offers enhanced visualization of architectural distortion and multiple masses. She stated that it was a different than routineHHUS imaging— the coronal plane allows for anatomic depiction of whole breast from skin to chest wall.
She addressed specific components radiologists need to look for with the coronal plane. Her recommendations include: Alterations in the tissue: dark/black holes; Identify masses, architectural distortion,spiculation— lesion analysis; look at surrounding tissue (echogenicity, desmoplastic reaction); and spiculation/retraction similar to that seen on 2D and DBT mammography. She also noted the multi-slice coronal view being used more regularly in her practice, as they continue looking at anatomy and identifying abnormalities.
人工智能在成功实施过程中有作用吗?她相信有。斯皮尔认为,人工智能工具可以以多种方式帮助放射科医生,从提高生产力,到让放射科医生更快地专注于潜在的兴趣领域。她补充说,人工智能可能会影响一个人的准确性,因为人工智能算法有很高的灵敏度。
“Relying on AI is a good thing to do to balance the quality of interpretation and cancer detection,” noted Spear.
She identified four primary benefits of AI in discussing its role in successful implementation. AI tools assist the radiologist first and foremost, she noted. It increases productivity by allowing a view of the entire case at-a-glance; third, users are drawn to focus attention on potential areas of interest, which leads to increased confidence; and lastly, accuracy, as AI algorithms detect and mark easy-to-miss lesions and oversights with high sensitivity.
“We are always asking what we can do to improve efficiency and success,” said Spear, reporting that “The specificity is wonderful, and new users and experienced users can both benefit.” Noting how increased volumes of screenings lead to reader fatigue, she reinforced the benefit that this helps radiologists hone in on abnormalities, and provide a confidence boost on imaging so radiologists can readily work through images for better outcomes.
斯皮尔在结束语中说:“我们在自动超声方面的经验促使我们理解成功的策略。”
She outlined that AUS implementation strategies rely on workflow planning/IT, integration/scheduling, and an emphasis on small group training. AUS interpretation strategies rely upon high quality imaging, optimizing software utilization, understanding AUS technology and particularly understanding the role of the coronal plane, andreduction of false positives.Spear表示:“在我们看来,人工智能是我们未来实践的关键组成部分。
“在如此繁忙的实践中,我们理解任何模式的实施在最初都将面临艰巨的挑战,但它始终是关于在过程中增加价值。总的来说,作为医生和放射科医生,我们在我们的环境中感到舒适,所以改变是困难的。一开始我们选择了四个人,并且取得了成功。在我们反复解释策略之后,我们发现了一些我们之前没有看到的东西。立体是一个优势,这一点我们已经知道了。这是人之常情,但必须坚持不懈。最重要的是要慢慢开始,并且有一个医生来支持这个项目。QView CAD是最近增加的实践,现在它与ABUS工作站集成,我们正在努力传播它的全面。”
Recounting an experience that impacted her, she shared one instance where she had worked with one woman from the start of her diagnosis. Noting how rare it is to get feedback, she recalled that after treatment and recovery, the patient came to her practice and gave her a clock, to thank Spear for giving her back the gift of her time.
“This helps propel you to find new and better ways of doing things and improving
the status quo,” concluded Spear.
Related ABUS content:
Driving the Adoption of ABUS With AI Technology
QView Medical Showcases QVCAD for ABUS Exams at RSNA 2018
Artificial Intelligence Helps Detect Breast Cancer and Saves Time
FDA Proposes New Rules for Mammography Reporting and Quality Improvement

 August 11, 2022
August 11, 2022